

US/UK social security, work and health


Is there a relationship between the social security offer and levels of economic inactivity due to ill health?
This may be a difficult question to ask because it can appear accusatory that people are ‘working the system’. It is a difficult question to answer, mainly due to the lack of clear comparators or counterfactuals.
Policy Exchange’s recently published ‘Not Fit for Purpose’ report begins to interrogate the link between sickness certification and welfare. The report cites the OBR’s finding that ‘a causal link between welfare and inactivity might arise due to changes in some combination of the generosity of support (relative to unemployment benefits), their degrees of conditionality, the functioning of the assessment regimes, and the extent of back-to-work support provided to people on health-related benefits.’ Policy Exchange’s report also draws together evidence highlighting that monthly onflows for incapacity benefits have nearly trebled since 2017, and that the incapacity approval rate of around 70% since 2015 is nearly double what it was in its first year of operation.
Incentives do matter and play into the psychosocial element of fitness for work which can have a significant impact on function. For example, on an individual basis, an employee’s occupational sick pay dropping after a certain period of time off can catalyse a recalibration of psychosocial factors leading to a genuine improvement in functioning, enabling return to work.
Compared to the UK, the US has a lower social security incapacity benefit safetynet with a higher threshold for access. Qualification for Social Security Disability Insurance (SSDI) depends on an individual earning enough credits through paying into the system when they were well enough to work. Supplemental Security Income (SSI) is based on financial need within or outside of the context of disability, rather than work history. This is more parallel to the UK’s health-related component of Universal Credit, which is means and need tested. Unlike the US, the UK also has exclusively needs tested disability benefits, such as Personal Independent Payment (PIP). PIP is designed to support with the extra cost of living with long term ill health and disability and therefore accessible to those that qualify on the basis of their health and function regardless of their means.
The other psychosocial driver to employment in the US vs the UK is that access to healthcare through insurance is built into employment compensation packages, often not just for the individual working but for their immediate family too. Meanwhile, the US benefits system segues into federal health insurance access. SSDI recipients qualify for Medicare after two years or sooner if they have certain disabilities. SSI claimants may be eligible for Medicaid immediately but this varies state to state and inevitably people fall through the cracks in coverage.
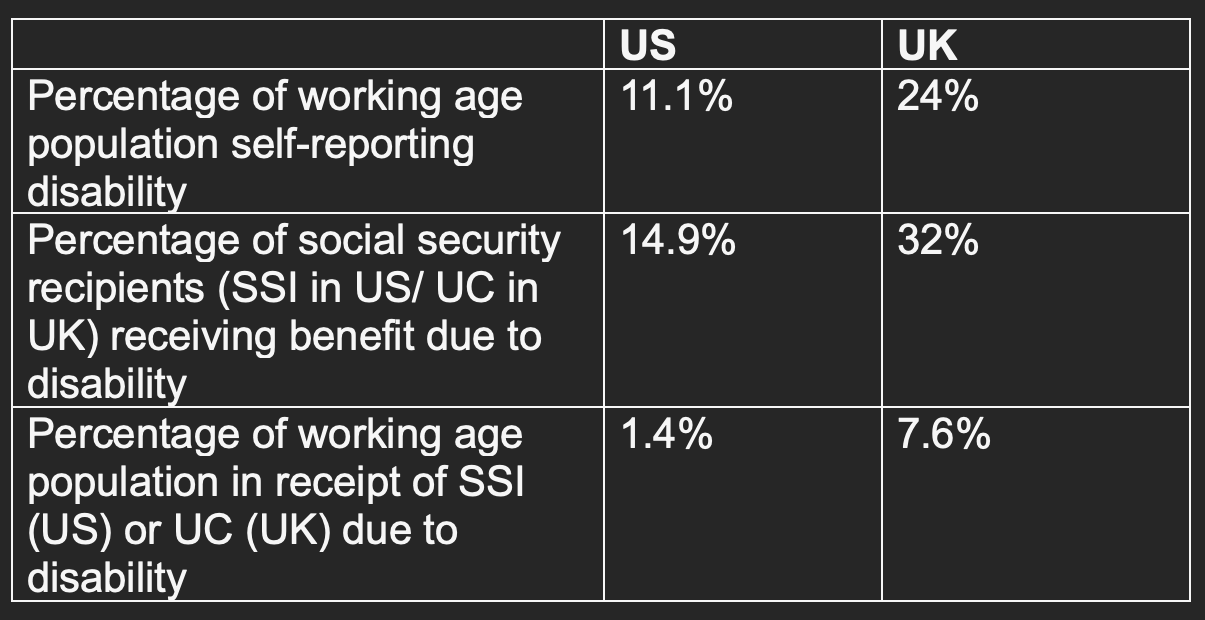
The work and health climate is so different in the US vs the UK that controlling for confounders is difficult when comparing data. It is also difficult to prepare data for comparison that has been collected in different ways across the two countries. However, is interesting to have a look at data on US vs UK working age population disability and benefit rates to give some indication on how these differences in societal infrastructure relate to work and health.
US vs UK disability and related social security rates
Lara’s take
Financial incentives around work and health definitely matter. And this is not to undermine any individual’s claim to benefits, rather that we must recognise that psychosocial context is really significant in the relationship between work and health. The contrasting data from the US vs the UK is striking and demonstrates that push and pull factors from social security into work are relevant and can make an impact. The stronger safety net in the UK compared to the US is a good thing for our society. But in order for this safety net to be effective we need to better understand how to leverage it to support people back into economic activity.
Hi Lara, another great review simplified. Great to have the transatlantic perspective since it seems to drive much of the government thinking. Interesting to see how much employee engagement is falling in the US(recent GAllup study), which is a sideways comment regarding benefits. I also wonder whether you are seeing evidence about the negative impact of poor access to timely treatment is as a moderator of inactivity especially with the ageing worker cohort. Investing in system improvements versus blaming the individual when things go wrong would appear to be a novel idea!